
ARISE, a clinical AI research team led by physician researchers from Stanford University School of Medicine and Harvard Medical School, recently published NOHARM (Numerous Options Harm Assessment for Risk in Medicine), one of the most comprehensive independent evaluations of clinical AI safety to date.
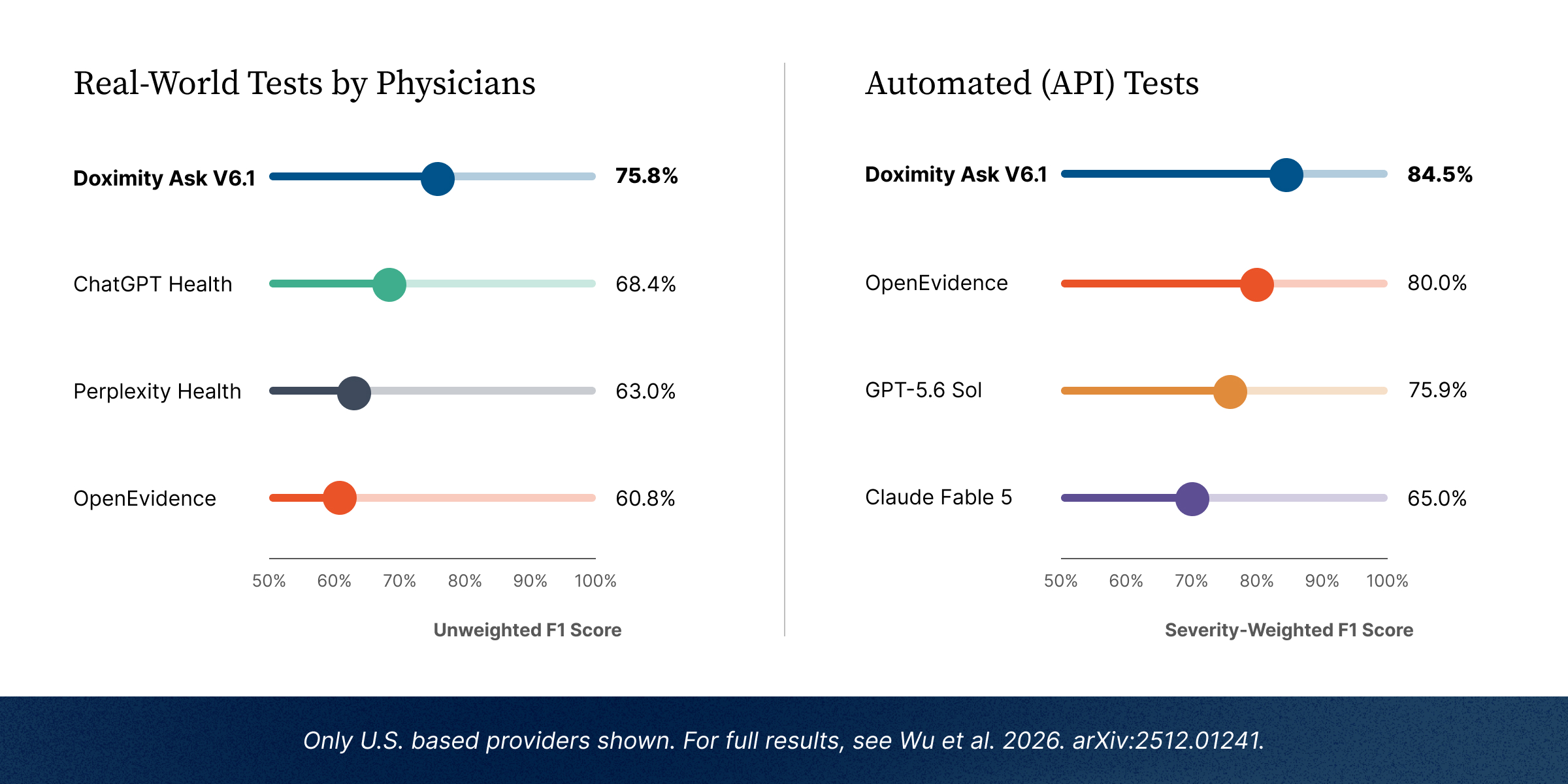
Developed by more than 50 researchers with contributions from 29 board-certified physicians, NOHARM evaluates how often AI-generated recommendations could result in patient harm across 1,100 physician-derived clinical scenarios spanning 10 medical specialties. Rather than measuring medical knowledge alone, it provides a rigorous framework for evaluating the safety of healthcare AI systems for real-world clinical decision support.
We are proud to share that Doximity Ask outperformed OpenEvidence, GPT-5.6 Sol, Claude Fable 5, and other leading frontier AI models. More broadly, the study found that clinically specialized AI systems consistently outperformed frontier general-purpose models, reinforcing the importance of building AI specifically for medicine rather than adapting general-purpose systems.
Why Doximity Ask Performs Differently
At Doximity, we have always believed that building trustworthy clinical AI requires more than powerful foundation models. It requires physician oversight, continuous learning, and accountability to real-world clinical outcomes. The findings from NOHARM reinforce that philosophy: success in clinical AI is about helping physicians make safer, more complete clinical decisions, not just answering medical questions.
The bar for clinical AI should be extraordinarily high. Doximity Ask, powered by PeerCheck™, is the only HIPAA-compliant AI platform where practicing physicians continuously review AI-generated answers for clinical accuracy, evidence quality, completeness, and potential bias.
Those reviews do more than improve individual responses. Every physician edit becomes structured feedback that improves future answers across the platform, enabling the system to learn from expert clinical judgment at scale. That continuous learning is especially important because NOHARM found that the most serious AI failures resulted from omitted clinical recommendations rather than incorrect ones. Physician review helps identify those gaps and reinforces more complete clinical reasoning over time.
Evidence-first clinical reasoning
Doximity Ask is built on an evidence-first architecture that uses current, peer-reviewed sources as the foundation for every response, rather than relying solely on static model memory. At query time, the system identifies the clinical question and retrieves the most relevant literature from a continuously updated index of millions of peer-reviewed publications and specialty society guidelines, refreshed daily.
For complex patient scenarios requiring multi-step clinical decision-making, Ask uses agentic reasoning to break problems into structured steps and generate clinically grounded recommendations informed by medical calculators, structured drug information, and evidence-based reasoning.
The platform is HIPAA compliant and includes end-to-end encryption, role-based access controls, audit logging, and session isolation. Learn more.
Beyond Benchmarks: Real-World Clinical Adoption
Independent benchmarks are important, but so is real-world adoption.
Today, Doximity's Clinical AI Suite has been reviewed, approved, and deployed across more than 150 health systems, including eight of the top 20 hospitals in the United States. We believe widespread clinical adoption, together with rigorous independent evaluation, provides a more complete picture of whether AI systems have earned physicians' trust.
Raising the Bar for Clinical AI
NOHARM reflects an important shift in how healthcare AI should be evaluated. The question is no longer simply whether an AI system can answer medical questions correctly, but whether those recommendations are consistently safe for patients.
As independent evaluations become more rigorous, meaningful differences between clinical AI systems are becoming increasingly visible. That transparency benefits physicians, healthcare organizations, and ultimately patients.
We view this recognition not as a finish line, but as independent validation of the approach we have invested in from the beginning: physician-reviewed AI, continuously improved through PeerCheck™, grounded in current medical evidence, and built for real clinical practice.